Understanding Postnatal Depression: The Australian Reality
Postnatal depression (PND), also known as postpartum depression, is a significant mental health condition affecting new mothers during one of the most transformative periods of their lives. Far from being a sign of weakness or inadequate mothering, PND is a medical condition that requires understanding, support, and appropriate treatment.

Australian Prevalence and Statistics
Recent Australian research reveals the true scope of perinatal mental health challenges:
- 3.3% of Australian mothers experience postnatal depression in major metropolitan areas (based on NSW Health District data)
- Up to 20% of women experience anxiety, depression, or stress during the perinatal period (pregnancy and first year postpartum)
- 6.2% prevalence of antenatal depression during pregnancy
- Culturally and linguistically diverse (CALD) women show higher rates (4.2% vs 3.3% in general population)
- Only 45-55% of affected mothers receive a professional diagnosis
During the COVID-19 pandemic, Australian research found even higher rates:
- 26.5% of pregnant women reported clinically significant depressive symptoms
- 19% of postnatal women experienced elevated depression during pandemic periods
These statistics highlight that postnatal depression is far more common than many realize, particularly in Australia’s diverse population.
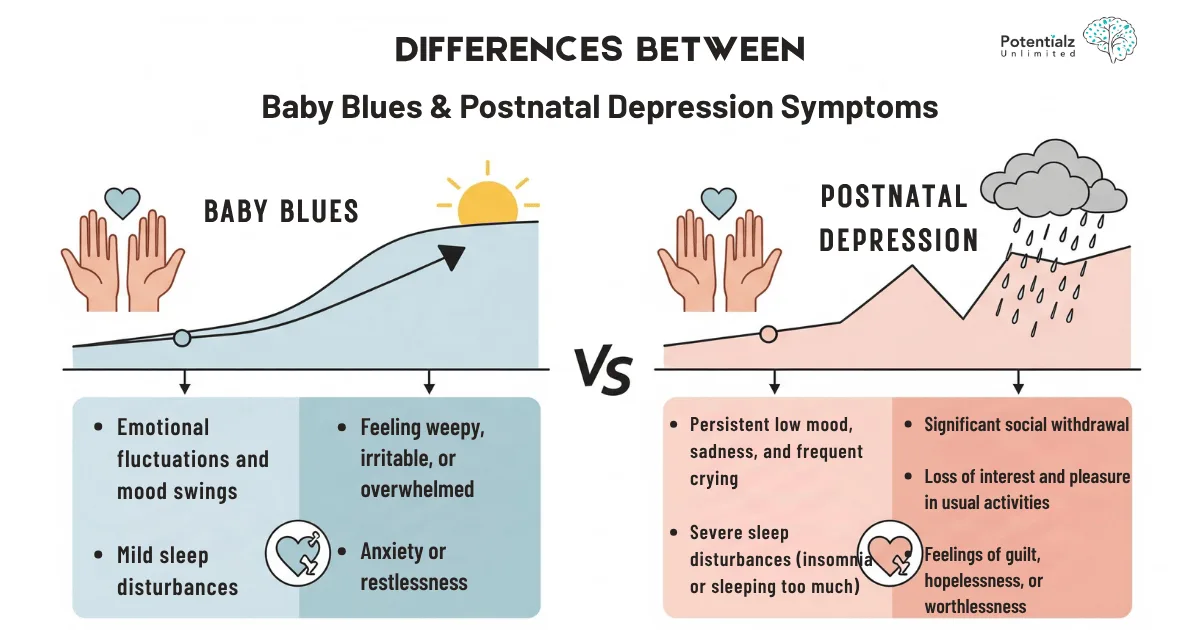
Beyond the ‘Baby Blues’
It’s crucial to distinguish between the common ‘baby blues’ and clinical postnatal depression:
Baby Blues (affects up to 80% of new mothers):
- Occurs within the first 10 days after birth
- Mild mood changes, tearfulness, and anxiety
- Resolves naturally without treatment
- Lasts only a few days
Postnatal Depression:
- Can occur any time within the first 12 months after birth
- Persistent symptoms lasting weeks or months
- Significantly impacts daily functioning and bonding
- Requires professional support and treatment
“UP TO 1 IN 5 WOMEN EXPERIENCE ANXIETY AND/OR DEPRESSION DURING PREGNANCY, AND/OR FOLLOWING BIRTH.”
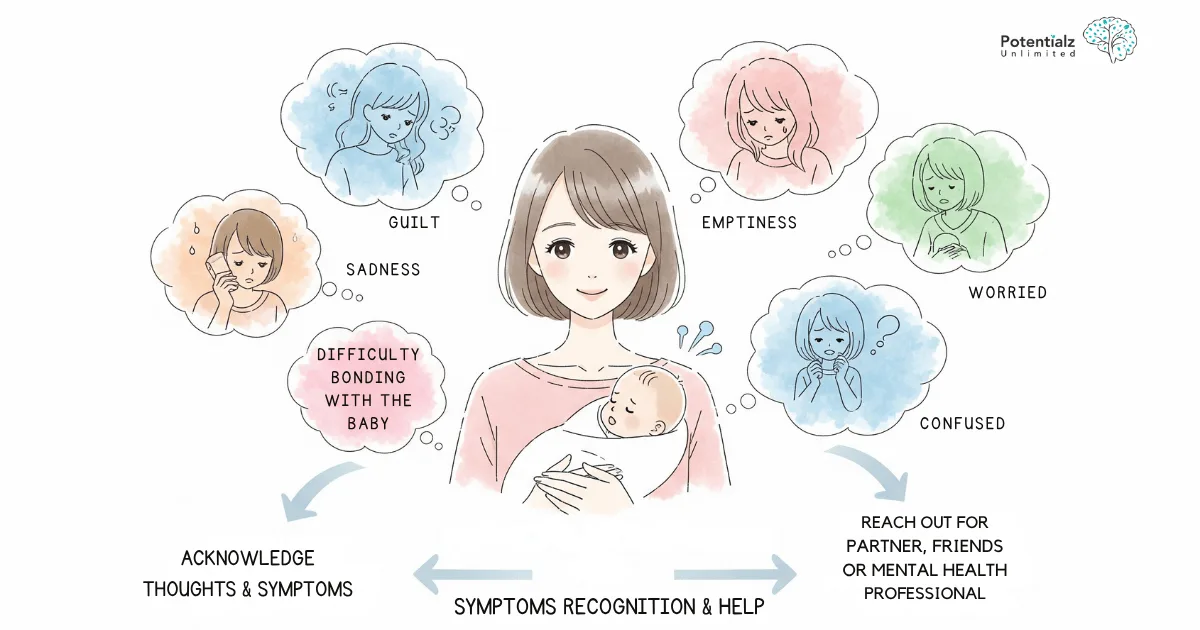
Recognizing the Signs and Symptoms
Understanding the signs of postnatal depression is crucial for early identification and intervention. The symptoms can vary significantly between individuals but typically include:
Emotional Symptoms
- Persistent sadness or low mood that doesn’t lift
- Loss of interest or pleasure in activities once enjoyed, including time with baby
- Overwhelming feelings of guilt or inadequacy as a mother
- Excessive worry or anxiety about the baby’s health or your ability to care for them
- Feeling emotionally numb or disconnected from your baby
- Mood swings that feel uncontrollable
- Feelings of hopelessness about the future
Physical Symptoms
- Sleep disturbances beyond normal newborn-related sleep loss
- Appetite changes - either loss of appetite or overeating
- Fatigue and low energy that rest doesn’t relieve
- Physical aches and pains without apparent cause
- Restlessness or sluggishness
Cognitive Symptoms
- Difficulty concentrating or making decisions
- Memory problems beyond normal ‘baby brain’
- Recurring negative thoughts about yourself or your baby
- Worry about harming yourself or your baby
- Thoughts of death or suicide
Behavioral Symptoms
- Withdrawal from family and friends
- Avoiding baby-related activities or social situations
- Difficulty bonding with your baby
- Increased irritability or anger
- Crying frequently or inability to cry at all
Warning Signs Requiring Immediate Help
If you experience any of the following, seek immediate professional support:
- Thoughts of harming yourself or your baby
- Severe confusion or disorientation
- Hallucinations or delusions
- Inability to care for yourself or your baby
- Panic attacks that feel uncontrollable
Risk Factors and Vulnerable Populations
Australian research has identified several factors that increase the likelihood of developing postnatal depression:
Demographic Risk Factors
- Cultural and linguistic diversity: CALD women show higher rates (8.0% antenatal, 4.2% postnatal)
- Socioeconomic disadvantage: Lower socioeconomic status increases risk
- Young maternal age: Particularly under 25 years
- Single motherhood: Lack of partner support significantly increases risk
- Geographic isolation: Rural and remote areas with limited support services
Psychological Risk Factors
- Previous mental health history: Depression, anxiety, or other mental health conditions
- Lack of social support: Weak support networks or family conflict
- Relationship problems: Poor partner relationship or domestic violence
- Unplanned pregnancy: Ambivalence about pregnancy or motherhood
- Birth trauma: Difficult birth experience or emergency cesarean
Medical Risk Factors
- Pregnancy complications: Gestational diabetes, pre-eclampsia, or other complications
- Premature birth or infant health problems
- Breastfeeding difficulties
- Hormonal factors: Particularly rapid hormonal changes postpartum
- Sleep deprivation: Severe disruption beyond normal newborn sleep patterns
Australian-Specific Vulnerabilities
Research in Australian healthcare settings has highlighted particular challenges:
For CALD Communities:
- Language barriers affecting access to services
- Cultural stigma around mental health
- Different cultural expectations of motherhood
- Limited culturally appropriate support services
For Rural and Remote Areas:
- Geographic isolation from specialist services
- Limited mental health resources
- Reduced social support networks
- Economic pressures related to agricultural communities
For Indigenous Australian Women:
- Complex historical and cultural factors
- Need for culturally appropriate assessment tools
- Traditional healing approaches alongside Western medicine
- Community-based support models
Evidence-Based Treatment Approaches
Cognitive Behavioral Therapy: The Gold Standard
Extensive research demonstrates that Cognitive Behavioral Therapy (CBT) is one of the most effective treatments for postnatal depression. A comprehensive meta-analysis of 79 randomized controlled trials found that CBT was effective for perinatal maternal depression in both short-term and long-term outcomes.
How CBT Works for Postnatal Depression:
CBT operates on the principle that our thoughts, feelings, and behaviors are interconnected. In postnatal depression, negative thought patterns about mothering abilities, self-worth, and the future can create a cycle of depression and anxiety.
Key CBT Components for New Mothers:
1. Psychoeducation
- Understanding postnatal depression as a medical condition
- Learning about normal adjustment to motherhood
- Recognizing the relationship between thoughts, feelings, and behaviors
- Understanding how hormonal changes affect mood
2. Cognitive Restructuring
- Identifying negative automatic thoughts (“I’m a terrible mother”)
- Challenging unrealistic or catastrophic thinking
- Developing more balanced, realistic thoughts
- Addressing perfectionist expectations about motherhood
3. Behavioral Activation
- Gradually increasing pleasant activities
- Setting achievable daily goals
- Improving self-care routines
- Enhancing social connections and support
4. Problem-Solving Skills
- Breaking down overwhelming tasks into manageable steps
- Developing coping strategies for common challenges
- Improving communication with partners and family
- Managing practical aspects of new motherhood
5. Relapse Prevention
- Identifying early warning signs
- Developing a personal coping plan
- Building long-term support networks
- Preparing for future life changes
Research Evidence for CBT Effectiveness:
Recent meta-analyses demonstrate compelling evidence:
- Short-term effectiveness: CBT showed significant improvement (SMD -0.69) compared to control groups
- Long-term benefits: Effects maintained at follow-up (SMD -0.59)
- Anxiety reduction: CBT also effective for perinatal anxiety (SMD -0.63)
- Multiple formats: Effective whether delivered individually, in groups, or online
Australian CBT Programs and Services
MumMoodBooster Program
Developed specifically for Australian mothers, this evidence-based online CBT program has been tested in randomized controlled trials. The program includes:
- 9 structured sessions addressing maternal mood
- Behavioral activation techniques
- Cognitive strategies for negative thinking
- Self-esteem building exercises
- Partner support components
Getting Ahead of Postnatal Depression
An Australian-developed manualized CBT program showing effectiveness in multiple trials:
- Specifically designed for postnatal depression
- Culturally adapted for Australian context
- Available through many Australian psychology services
- Combines individual and group delivery options

Interpersonal Therapy (IPT)
IPT focuses on improving relationships and addressing interpersonal issues that may contribute to depression. For new mothers, this often involves:
- Role transitions: Adjusting to motherhood and changing identity
- Relationship conflicts: Managing changes in partnership and family dynamics
- Social support: Building and maintaining supportive relationships
- Communication skills: Expressing needs and concerns effectively
Research shows IPT is particularly effective when relationship issues are primary contributors to depression.
Online and Digital Interventions
Given the challenges new mothers face accessing traditional therapy, online interventions have become increasingly important:
Advantages of Online CBT:
- Accessible from home while caring for baby
- Flexible timing around feeding and sleeping schedules
- Anonymous and private
- Lower cost than face-to-face therapy
- Available in rural and remote areas
Research Findings:
A systematic review of 18 studies involving 3,689 women found online CBT effective for postpartum depression, with optimal results when:
- Total intervention duration was 9+ weeks
- 12 or fewer total sessions provided
- Professional guidance included
- Delivered via website or video conferencing platforms
Accessing Help in Australia
Medicare Support for Postnatal Depression
Australia’s healthcare system provides substantial support for maternal mental health:
Mental Health Treatment Plans
- Up to 10 psychology sessions per calendar year with Medicare rebates
- Higher rebates for clinical psychologists ($145.25 vs $98.95 for registered psychologists)
- No out-of-pocket costs with bulk-billing providers
- Telehealth options available Australia-wide
Perinatal-Specific Services
- Specialist perinatal mental health teams in major hospitals
- Mother-baby units for severe cases requiring inpatient care
- Perinatal psychiatrists for complex cases or medication management
- Maternal and child health nurses trained in mental health screening
Key Australian Support Organizations
PANDA (Perinatal Anxiety & Depression Australia)
- National Helpline: 1300 726 306 (Monday-Saturday)
- Multicultural support available in various languages
- Online resources and support groups
- Professional education and training programs
- Aboriginal and Torres Strait Islander specific support
COPE (Centre of Perinatal Excellence)
- Evidence-based treatment programs
- Online therapy platforms
- Professional training for healthcare providers
- Research and advocacy for perinatal mental health
- Multilingual resources
Beyond Blue
- 24/7 Support Line: 1300 22 4636
- Online chat support
- Comprehensive information about postnatal depression
- Find a therapist directory
- Workplace support programs
State-Based Services
New South Wales
- Karitane: Residential and day programs for mothers and babies
- Tresillian: Family care centers with mental health support
- NSW Health Perinatal Mental Health Network
Victoria
- Royal Women’s Hospital: Specialized perinatal mental health services
- Austin Health: Mother-baby units
- Mercy Health: Integrated perinatal care
Queensland
- Mater Mothers’ Hospital: Perinatal mental health programs
- Metro North Health: Community perinatal mental health teams
Western Australia
- King Edward Memorial Hospital: Perinatal mental health services
- Ngala: Family support services including mental health
South Australia
- Women’s and Children’s Hospital: Perinatal psychiatry services
- Catherine House: Specialized women’s mental health support
Rural and Remote Support
Telehealth Services
- Medicare-subsidized video consultations with psychologists
- Specialist perinatal psychiatry via telehealth
- Online support groups connecting rural mothers
Flying Doctor Service Mental Health
- Rural mental health programs
- Emergency mental health response
- Training for local health providers
Regional Health Networks
- Local health districts with perinatal mental health coordinators
- Mobile mental health services
- Community health centers with maternal support
Medication Considerations During Breastfeeding
For some women, medication may be an important component of treatment, particularly for moderate to severe postnatal depression.
Safe Medication Options
Australian guidelines recommend several medications considered safe during breastfeeding:
First-Line Antidepressants:
- Sertraline (Zoloft): Minimal transfer to breast milk
- Paroxetine (Aropax): Low levels in breast milk
- Fluoxetine (Prozac): Generally safe but requires monitoring
Second-Line Options:
- Citalopram (Cipramil): Low levels in breast milk
- Escitalopram (Lexapro): Minimal infant exposure
- Venlafaxine (Efexor): May be used with monitoring
Important Considerations
- Consult with your GP or psychiatrist before starting any medication
- Benefits vs. risks assessment includes severity of depression
- Breastfeeding continuation is usually possible with most medications
- Monitor infant for any changes in feeding, sleeping, or behavior
- Regular review ensures optimal dosing and effectiveness
Non-Medication Alternatives
For mothers preferring non-pharmaceutical approaches:
- Intensive CBT or IPT
- Support group participation
- Peer support programs
- Lifestyle interventions (exercise, nutrition, sleep hygiene)
- Complementary therapies (with professional guidance)
Self-Care Strategies and Lifestyle Support
While professional treatment is often essential, self-care strategies can significantly support recovery:
Physical Wellness
- Gentle exercise: Even 10-minute walks with baby can improve mood
- Nutrition: Regular, nutritious meals support brain chemistry
- Sleep hygiene: Rest when baby sleeps, create calming bedtime routines
- Sunlight exposure: Natural light helps regulate mood and sleep cycles
Emotional Wellness
- Mindfulness and meditation: Apps like Headspace or Calm offer postnatal programs
- Journaling: Recording thoughts and feelings can provide clarity
- Creative expression: Art, music, or writing as emotional outlets
- Gratitude practice: Daily noting of positive moments, however small
Social Connection
- New parent groups: Connect with other mothers in your area
- Family support: Accept help with household tasks and baby care
- Maintain friendships: Schedule regular check-ins with supportive friends
- Partner communication: Share feelings and needs openly
Practical Support
- Lower expectations: Adjust standards for housework and daily tasks
- Accept help: Allow others to assist with cooking, cleaning, and errands
- Time management: Prioritize essential tasks and rest
- Professional support: Consider hiring help for cleaning or meal preparation

Supporting a Partner or Loved One
Partners, family members, and friends play crucial roles in recovery from postnatal depression:
How to Help
- Listen without judgment: Provide a safe space for expressing feelings
- Offer practical support: Help with baby care, household tasks, and errands
- Encourage professional help: Support seeking treatment without pressure
- Learn about postnatal depression: Understand it’s a medical condition, not a choice
- Be patient: Recovery takes time and may involve setbacks
What NOT to Do
- Minimize feelings: Avoid saying “just think positive” or “other mothers cope”
- Take it personally: Remember that withdrawal isn’t about you
- Give unsolicited advice: Focus on listening rather than problem-solving
- Expect quick fixes: Understand that recovery is a gradual process
- Ignore warning signs: Take any mentions of self-harm seriously
When to Seek Emergency Help
Contact emergency services (000) if someone:
- Expresses thoughts of harming themselves or their baby
- Shows signs of psychosis (hallucinations, delusions)
- Is unable to care for themselves or their baby
- Has made any attempt at self-harm
Partner Depression
Research shows that 1 in 10 fathers also experience paternal depression during the perinatal period. Partners need support too and should seek help if experiencing:
- Persistent sadness or anxiety
- Withdrawal from family
- Difficulty bonding with baby
- Changes in sleep, appetite, or energy
- Irritability or anger
Recovery and Long-Term Wellness
What Recovery Looks Like
Recovery from postnatal depression is possible and common. With appropriate treatment:
- 80% of women experience significant improvement
- Symptoms typically improve within 3-6 months of treatment
- Most mothers develop strong bonds with their babies
- Treatment skills help manage future life stresses
- Family relationships often strengthen through the recovery process
Timeline Expectations
Weeks 1-4: Beginning Treatment
- Initial assessment and treatment planning
- Starting therapy or medication
- Building support networks
- Possible initial increase in emotional awareness
Weeks 4-12: Active Treatment
- Regular therapy sessions
- Implementing coping strategies
- Gradual improvement in mood and energy
- Better sleep patterns and self-care
Weeks 12-24: Consolidation
- Significant improvement in symptoms
- Stronger mother-baby bonding
- Increased confidence in parenting
- Preparation for treatment conclusion
6+ Months: Maintenance
- Occasional check-ins with healthcare providers
- Continued use of learned strategies
- Strong family relationships
- Ability to manage normal life stresses
Preventing Future Episodes
- Regular mental health check-ups during subsequent pregnancies
- Early intervention strategies if symptoms emerge
- Strong support networks maintained over time
- Stress management techniques applied to daily life
- Self-awareness of early warning signs
Building Resilience
- Developing coping skills that extend beyond motherhood
- Creating meaningful connections with other parents
- Finding purpose and identity beyond being a mother
- Maintaining physical and emotional wellness as priorities
- Seeking help early for any mental health concerns
Breaking the Stigma
Common Myths vs. Reality
- Myth: “Good mothers don’t get depressed” Reality: Postnatal depression is a medical condition unrelated to mothering ability
- Myth: “It’s just hormones and will pass” Reality: While hormones play a role, PND requires professional treatment
- Myth: “Taking medication means you’re weak” Reality: Medication can be essential for recovery and doesn’t reflect personal strength
- Myth: “You should be grateful and happy” Reality: Gratitude and depression can coexist; feelings are complex
- Myth: “It only affects first-time mothers” Reality: PND can occur after any pregnancy, regardless of previous experiences
Creating Supportive Communities
- Open conversations about maternal mental health normalize seeking help
- Sharing recovery stories provides hope to struggling mothers
- Education in workplaces supports returning mothers
- Healthcare provider training improves detection and referral
- Policy advocacy ensures adequate mental health resources
Test Your Knowledge
Key Takeaways: Your Journey to Recovery Starts Here
Bottom Line Up Front
Postnatal depression is a common, treatable medical condition affecting 1 in 5 Australian mothers. With proper support and evidence-based treatment, complete recovery is not only possible but expected. You are not alone, and help is readily available through Australia’s comprehensive healthcare system.
Essential Understanding
- Postnatal depression is medical, not personal - it’s not a reflection of your mothering ability or character
- Treatment is highly effective - 80% of women experience significant improvement with appropriate support
- Australia offers excellent support - from Medicare-subsidized therapy to specialized perinatal services
- Recovery strengthens families - getting help benefits not just you, but your baby and entire family
- You deserve support - seeking help is an act of love for yourself and your child
Your Action Steps
- If you’re struggling: Contact PANDA helpline (1300 726 306) or see your GP this week
- If supporting someone: Listen, learn, and encourage professional help without judgment
- For ongoing wellness: Build support networks and prioritize self-care as part of good mothering
- Spread awareness: Share information to help other mothers recognize they’re not alone
Remember
Your mental health matters. Your wellbeing matters. You matter. Postnatal depression is temporary, treatable, and does not define your worth as a mother. With the right support, you can not only recover but discover strength and resilience you never knew you had.
Recovery is a journey, not a destination. Take it one day at a time, celebrate small victories, and know that brighter days are ahead.
References
- Australian Institute of Health and Welfare. (2024). Perinatal mental health in Australia. Retrieved from https://www.aihw.gov.au/reports/mothers-babies/perinatal-mental-health-australia
- Giallo, R., Cooklin, A., Zaat, T., D’Esposito, F., Crawford, S., Westrupp, E., & Nicholson, J. M. (2018). Determinants of antenatal depression and postnatal depression in Australia. BMC Psychiatry, 18(1), 49.
- Health Direct Australia. (2024). Postnatal depression. Retrieved from https://www.healthdirect.gov.au/postnatal-depression
- Milgrom, J., Danaher, B. G., Seeley, J. R., Holt, C. J., Holt, C., Ericksen, J., … & Gemmill, A. W. (2021). Internet and face-to-face cognitive behavioral therapy for postnatal depression compared with treatment as usual: Randomized controlled trial of MumMoodBooster. Journal of Medical Internet Research, 23(12), e17185.
- PANDA (Perinatal Anxiety & Depression Australia). (2024). Support for perinatal mental health. Retrieved from https://www.panda.org.au/
- Pettman, D., O’Mahen, H., Blomberg, O., Svanberg, A. S., von Essen, L., & Woodford, J. (2023). Effectiveness of cognitive behavioural therapy-based interventions for maternal perinatal depression: A systematic review and meta-analysis. BMC Psychiatry, 23(1), 208.
- Sockol, L. E. (2015). A systematic review of the efficacy of cognitive behavioral therapy for treating and preventing perinatal depression. Journal of Affective Disorders, 177, 7-21.
- Woolhouse, H., Gartland, D., Perlen, S., Donath, S., & Brown, S. J. (2020). Physical health after childbirth and maternal depression in the first 12 months post partum: Results of an Australian nulliparous pregnancy cohort study. Midwifery, 79, 102532.
- Yang, X., Ke, S., Gao, L. L., & Zhao, Y. (2022). Effectiveness of cognitive behavioral therapy for perinatal maternal depression, anxiety and stress: A systematic review and meta-analysis of randomized controlled trials. Clinical Psychology Review, 92, 102129.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.